By Tony Duffy and Mónica Lalanda
Future Healthcare Journal
Volume 13, Issue 1, March 2026, 100511
https://www.sciencedirect.com/science/article/pii/S2514664526000135
Under a Creative Commons license
Open access
Abstract
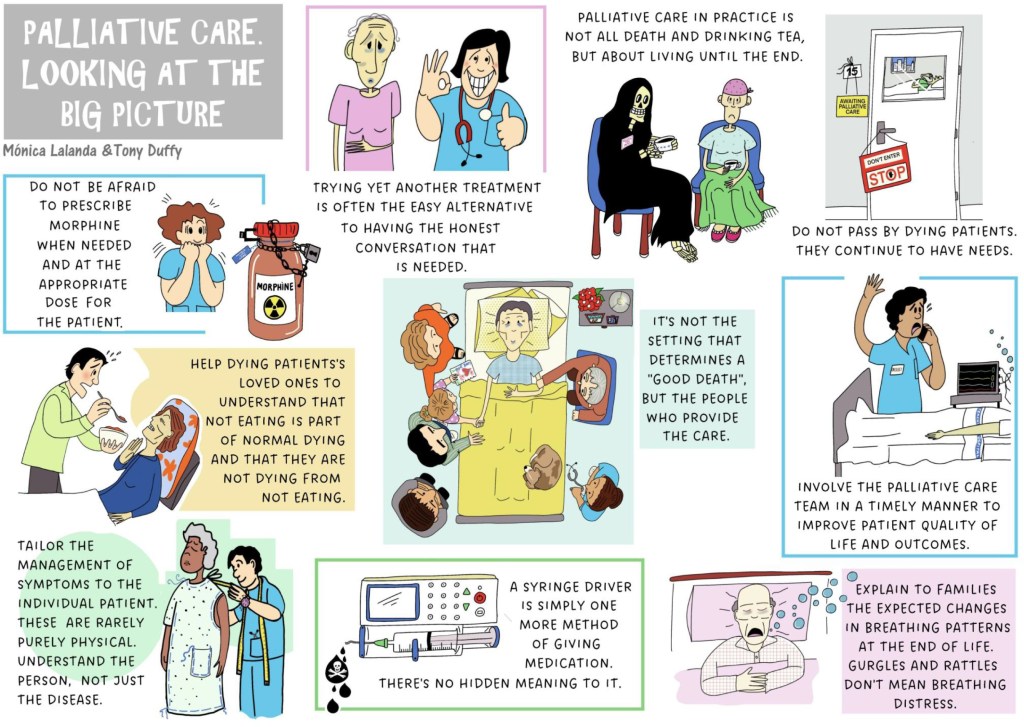
Despite decades of clinical practice, education and integration with other healthcare teams, palliative care remains enshrouded by myth and misconception. Through the powerful medium of comics, this article presents ten of the most misunderstood areas in palliative care. The topics explored were produced in conjunction with practising UK palliative care trainee doctors and realised to artistic form by a physician expert in graphic medicine. A novel infographic approach was carefully developed to be approachable yet thought-provoking. Each infographic is paired with content created to encourage reflection and provide applicable, real-world palliative care advice for all healthcare professionals. The historical connection between art and medicine is utilised in this modern article with the goal of improving patient care.
Graphic 1: Having honest conversations with patients
Not giving patients the information that they want and need when time is short can deprive them of opportunities to live that time in a way that matters most to them. There is evidence that patients value honest conversation even when their illness could shorten their life.1 Timely conversations help them plan and allow them to make the most of the time left.
Such conversations are difficult, even for the most experienced clinicians. Feelings of failing patients, clinical inadequacy, detachment and fear of saying the wrong thing are not uncommon. Using a structured approach to breaking bad news such as the SPIKES model and training via advanced communication courses can improve patient and clinician experiences.2,3 Ensure that the patient has the right people with them (some prefer to hear unwelcome news alone). Make sure you have support, too.
‘How long do I have?’ is often the first question people ask when given bad news. Providing overly specific time frames is fraught with peril. Should the patient die before this date, then the family can feel cheated. If the patient lives longer, they can feel terrified that they are on borrowed time or become doubtful that their diagnosis is correct. Approaching such questions in a qualitative rather than a purely quantitative manner can be helpful, exploring what the person may experience next with their illness and how this might affect them day to day.
Graphic 2: Timely palliative care is key
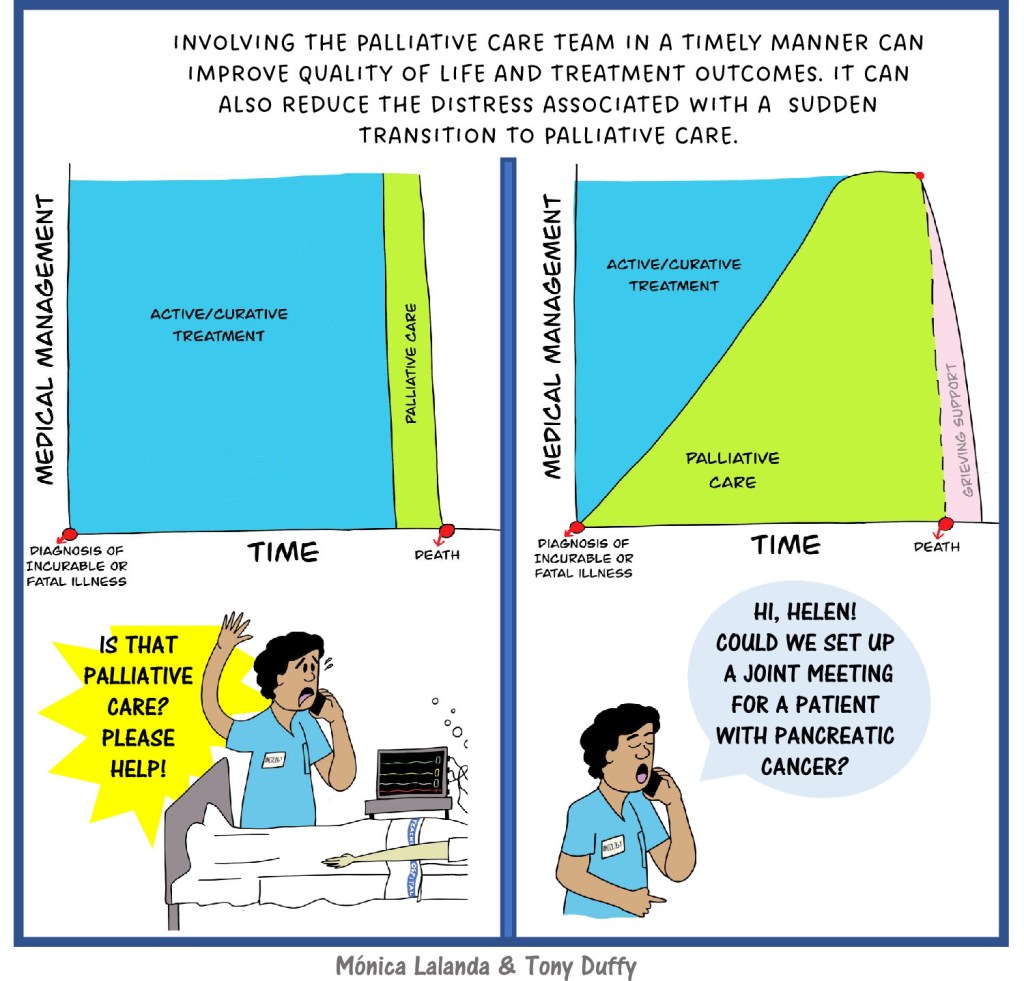
The ethos of palliative care is to improve the quality of life of patients and their families who are facing challenges associated with life-threatening illness, whether physical, psychological, social or spiritual.4 Note that there is no time frame or prognosis specified here. Palliative care may be a helpful addition at any phase of a person’s illness.
Earlier referrals give the best opportunity for people to understand and access all aspects of palliative care services to provide truly holistic care. With referrals close to end of life, the focus is often more medical due to the urgency of poorly controlled symptoms, and if there is a need for more rapid titration of medications so close to end of life, this can perpetuate the stereotype that palliative care clinicians come along and start ‘the morphine pump’. Timely referral gives the chance to understand who the patient is as a person, how the family unit interacts, and to address issues that may potentially escalate the patient’s distress.
Graphic 3: ‘Grim’ misconceptions about the palliative care clinician
Palliative care is poorly understood by the public (and often by our own medical and healthcare professional colleagues). Media imagery of deathbeds, handholding, elderly patients and hospital interiors overlook the co-existence of joy, humour and human connection even amid times of distress. Palliative care can be much more complex, gritty, even chaotic at times, as reflected in the Dying in the Margins project.5
Palliative care can be for anyone, at any age, in any setting. Child and young adult palliative care teams are nowhere to be seen in popular imagery; there is no indication of palliative care in residential care settings or representation of primary care work in the community. Are these standard images overcompensating to dispel the fear of terms like ‘death’, ‘dying’, ‘palliative care’ and ‘hospice’? The unease of the ‘Grim reaper team’ being involved remains, even among some healthcare professionals. Are you anxious about referring your patients?
While traditional palliative care models evolved to support cancer patients, up to 30% of patients now referred to specialist palliative care services have non-malignant conditions such as heart failure, COPD or neurodegenerative conditions. It is expected that palliative care demand will continue to rise for those with frailty, dementia and multimorbidity.6 The ethos of palliative care is universally transferrable and improves outcomes for patients and their loved ones regardless of the disease.7
Graphic 4: Tailoring symptom control to the individual
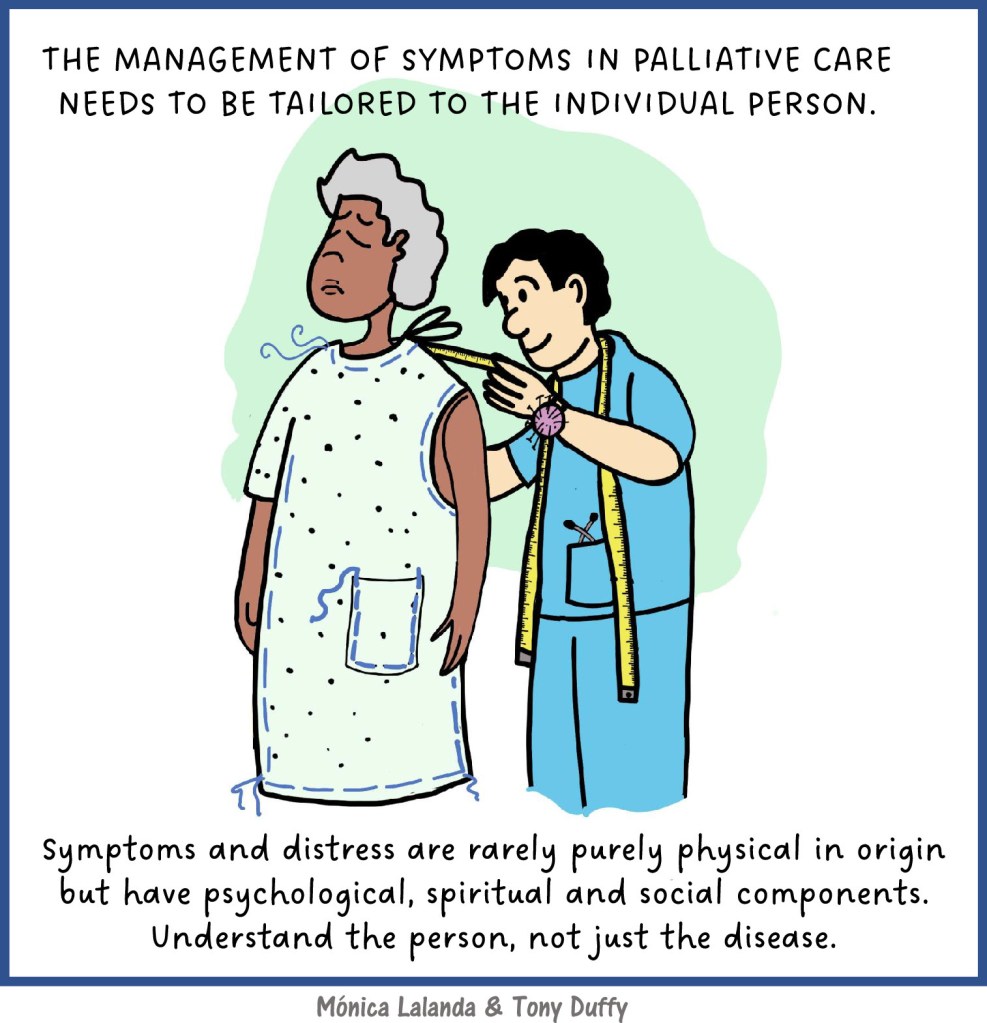
To prescribe in a truly patient-centred manner in palliative care, we must understand the root causes of patients’ distress. When prescribing for people who are frail, often with organ dysfunction and possibly already on several medications, we have a responsibility to understand the pharmacokinetics and pharmacodynamics of the drugs we use.
Physical symptoms do not exist in isolation. They are experienced by a person with unique biological make-up, life experiences, sociocultural background and spirituality. Medications mostly target receptors and biochemical pathways. There are no receptors to target that will change a person’s lived experience, isolation, guilt or existential distress in the face of life-limiting illness. When opioids do not reduce a person’s pain or anti-emetics fail to manage nausea, the origin of these experiences is often not only physical. Physical symptoms can be amplified by fear, anxiety, depression, loss of social role and connectedness to others.
We need to utilise the skills of a clinician that are often overshadowed by the focus on medical treatments – listening, compassion, acceptance and being non-judgemental – and to call upon the skills and experience of other MDT members. There may be a need to prompt discussion about rationalising medication that no longer benefits the patient. If changes are made, however, don’t forget to share that communication with all team members involved in the care of the patient.
Graphic 5: Even at end of life, daily reviews matter
Stepping into a room where a person is dying can be difficult, yet to provide support for people and their families at their most vulnerable is important and a privilege.
While skilled nursing care is no doubt the foundation of end-of-life care, physicians have a vital role in making sure that both prescribing and de-prescribing are effective and free from adverse effects. It is easy to forget the unpleasant withdrawal effects of stopping previous regular medications like gabapentin, opioids, anti-psychotics, beta-blockers and anti-epileptic drugs, not to mention nicotine or alcohol withdrawal as a cause of agitation at end of life. Deprescribing aids such as the OncPal guidance can help, but if in doubt, speak with the specialist who started the treatment.8
What practical help might we offer?
Use your clinical examination skills: check the patient’s mouth for dryness, ulcers or thrush. Do they still need that oxygen mask which covers their face or the painful heparin injections? Gently palpate the abdomen: urinary retention and constipation can cause restlessness towards end of life. Check for pressure damage on the ears, elbows and heels. Is there a need to rotate the subcutaneous injection sites due to redness?
Does the family have any questions? Encourage them to eat, drink and take some time for self-care, out of the room if possible.
Graphic 6: Morphine – much maligned
Misconceptions around the use of morphine and other opioids towards end of life remain common. When prescribed in a patient-specific manner and titrated appropriately, there is no evidence to show that opioids hasten death. Physical dependence is a naturally occurring phenomenon in everyone taking regular opioids; psychological dependence or addiction is rarely an issue with appropriate opioid prescribing in the last weeks of life, although care should still be taken in those with a longer prognosis and long-term pain.
The term ‘weak opioid’ in relation to codeine is a misnomer, as all opioids carry the same side-effects and risks. Approximately 10% of an oral codeine dose is metabolised by cytochrome CYP 2D6 to morphine to produce its analgesic effects. Poor metabolisers (up to 10% of the population) gain minimal pain relief, while ultra-rapid metabolisers (10–30% of people depending on ethnicity) and young children can produce dangerously high levels of morphine. The WHO three-step analgesic ladder with codeine on step two has been shown to be unnecessary when there is ready access to low-dose morphine. There are increasing numbers of opioid analgesics available, but morphine remains the first-line choice and has been shown to be safe, effective and cost-effective.9 Don’t forget that all opioids cause constipation, so concurrent prescription of a laxative is useful.
Graphic 7: Not eating and drinking at end of life is normal
When people are dying, their desire for nutrition wanes naturally; most people eventually become unable to eat or drink due to weakness and sleeping. This normal pattern is predictable and almost universal. Letting dying patients and their families know what to expect can help dispel significant distress. Concern over trying to ‘build the person up’, that they have ‘given up’ or that they are ‘starving to death’ are common.
Cancer cachexia is a syndrome of weight loss, fatigue and reduced appetite driven by underlying tumour-induced inflammation. Palliative care can play a significant role once the condition becomes refractory. Appetite loss may be present for months and progresses towards end of life. Concern and pressure from well-meaning people to eat more and regain weight can be frustrating for patients who themselves are rarely distressed by lack of food. Increasing food intake does not lead to sustained weight gain in advanced cachexia. An explanation of cachexia and providing some simple dietary counselling can make a difference. Giving the patient permission to eat and drink what they want, when they want in the last days/short weeks of life helps shift focus from sustenance to pleasure.10
Graphic 8: Place of death
Most people when asked would prefer to die in their own home, yet most people still die in hospital. Deaths in hospital are often viewed in a negative light or even a failure, but for many people, hospital is still the right place to die. For some people, admission to hospital at end of life is unavoidable due to family distress, symptom burden or 24-h social care gaps. Despite the pressured, noisy, exposed environment of the hospital, there are countless daily examples of excellent end-of-life care.
At home, it is often the person’s family who are the main carers, with healthcare professionals playing a supporting role. This reality for family members should be discussed honestly. Medication changes happen more slowly at home, and there may be delays in symptom management that cause distress. Beware of creating a ‘hospital’ environment by using too much medical kit. Continuity of care is a powerful tool: it is important that the patient and their family know exactly who to contact for help at all times. This lifeline list of numbers should go home with the patient when discharged from hospital.
Graphic 9: The syringe driver dilemma
Administration of medications via continuous subcutaneous infusion (CSCI) is an alternative to using the intravenous route in people who are unable or too sleepy to swallow, and some medications are normally used primarily in injectable form. Typically, the goal of CSCI is to provide consistent background control of symptoms such as pain, breathlessness, seizures, nausea and agitation, by mimicking the effects of taking regular medication orally. There is no real difference in effect between giving someone 20 mg of modified release oral morphine per day and an equivalent, carefully calculated amount per day via a syringe driver. A wide range of medications can be given subcutaneously, not just opioids and midazolam. Use of CSCI can provide excellent symptom control and reduce the need for frequent nursing input to administer injections. Some patients on a syringe driver are still able to walk, dress, socialise and even work. Remember when discharging someone from hospital who is using a syringe driver, this needs timely liaison with their local community services to ensure that it is replenished on an ongoing basis.
Graphic 10: Secretions at end of life
Changes in breathing are often a reliable indication that someone is nearing the end of their life. This can take the form of Cheyne–Stokes respiration, shallow breaths, rapid respiratory rate or pauses in breathing.
In an otherwise quiet room, it is hard for onlookers not to focus on the unusual pattern and noise of the dying person’s breathing. Some breathing pauses may last for over a minute, which can cause consternation if not explained. The build-up of small volumes of saliva or respiratory secretions in the upper airways is normal as people are dying. They do not have the ability to swallow, so respirated air cause crackles and rattles.
There remains a lack of evidence to support the use of anti-cholinergic drugs for the reduction of secretions at end of life.11 Their use at the very onset of noise appears to offer more benefit in some people.12 These drugs remain widely used, often in repeated doses, as there is a wish to relieve the distress of bedside companions, although the patient is usually otherwise settled. Gentle repositioning to one side or superficial suctioning by a trained person can be more effective for clearing secretions in some people. It is important to explain what is happening and that we cannot always remove the noises.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
CRediT authorship contribution statement
Tony Duffy: Writing – review & editing, Writing – original draft, Visualization, Methodology, Investigation, Conceptualization. Monica Lalanda: Writing – review & editing, Writing – original draft, Visualization, Methodology, Investigation, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
A great many thanks goes to the palliative care trainee doctors who contributed their time and ideas in the online brainstorming session during the preparation of this article. To Dr Kathryn Mannix for giving us her support and instilling her passion into this project, you are an inspiration to so many.
References
- 1R.G. Hagerty, P.N. Butow, P.M. Ellis, S. Dimitry, M.H. TattersallCommunicating prognosis in cancer care: a systematic review of the literatureAnn Oncol, 16 (7) (2005), pp. 1005-1053, 10.1093/annonc/mdi211View PDFView articleView in ScopusGoogle Scholar
- 2W.F. Baile, R. Buckman, R. Lenzi, G. Glober, E.A. Beale, A.P. KudelkaSPIKES—a six-step protocol for delivering bad news: application to the patient with cancerOncologist, 5 (4) (2000), pp. 302-311, 10.1634/theoncologist.5-4-302View at publisherView in ScopusGoogle Scholar
- 3J. Barth, P. LannenEfficacy of communication skills training courses in oncology: a systematic review and meta-analysisAnn Oncol, 22 (5) (2011), pp. 1030-1040, 10.1093/annonc/mdq441View PDFView articleView in ScopusGoogle Scholar
- 4WHO. Definition of palliative care. https://www.who.int/news-room/fact-sheets/detail/palliative-care, 2020. Accessed 21 feb, 2026.Google Scholar
- 5N. Richards, S. Quinn, E. Carduff, M. GottDying in the margins: experiences of dying at home for people living with financial hardship and deprivationSSM – Qual Res Health, 4 (2024), Article 100414VolumeView PDFView articleView in ScopusGoogle Scholar
- 6S.N. Etkind, A.E. Bone, B. Gomes, et al.How many people will need palliative care in 2040? Past trends, future projections and implications for servicesBMC Med, 15 (1) (2017), p. 102, 10.1186/s12916-017-0860-2View at publisherView in ScopusGoogle Scholar
- 7K.L. Quinn, M. Shurrab, K. Gitau, et al.Association of receipt of palliative care interventions with health care use, quality of life, and symptom burden among adults with Chronic Noncancer illness: a systematic review and meta-analysisJAMA, 324 (14) (2020), pp. 1439-1450, 10.1001/jama.2020.14205Google Scholar
- 8J. Lindsay, M. Dooley, J. Martin, et al.The development and evaluation of an oncological palliative care deprescribing guideline: the ‘OncPal deprescribing guideline’Support Care Cancer, 23 (1) (2015), pp. 71-78, 10.1007/s00520-014-2322-0View in ScopusGoogle Scholar
- 9P.S. Bramati, E. BrueraThe end of the second step of the World Health Organization analgesic ladder?Ann Oncol, 33 (12) (2022), pp. 1212-1213View PDFView articleView in ScopusGoogle Scholar
- 10T. Duffy, M. KochanczykPractical cancer cachexia management in palliative care – a review of current evidenceCurr Opin Support Palliat Care, 17 (3) (2023), pp. 177-185, 10.1097/spc.0000000000000655View at publisherView in ScopusGoogle Scholar
- 11B. Wee, R. HillierInterventions for noisy breathing in patients near to deathCochrane Database Syst Rev, 2008 (1) (2008), Article CD005177, 10.1002/14651858.cd005177.pub2View at publisherView in ScopusGoogle Scholar
- 12H. Wildiers, C. Dhaenekint, P. Demeulenaere, et al.Atropine, hyoscine butylbromide, or scopolamine are equally effective for the treatment of death rattle in terminal careJ Pain Symptom Manage, 38 (1) (2009), pp. 124-133, 10.1016/j.jpainsymman.2008.07.007View PDFView articleView in ScopusGoogle Scholar
Cited by (0)
This article reflects the opinions of the author(s) and should not be taken to represent the policy of the Royal College of Physicians unless specifically stated.
© 2026 The Author(s). Published by Elsevier Ltd on behalf of Royal College of Physicians.

